When it comes to characterizing muscle function, it is important to consider the animal model’s phenotype and the main source of dysfunction. Many researchers ask, should I be stimulating the hindlimb muscle or muscle group directly to measure force? Or should I instead be stimulating the nerve and measuring resultant force production following the physiological pathway. This is an important question and one that we will discuss in this blog so you can ensure you are using the most appropriate method to measure hindlimb mechanics in your animal models.
Nerve Stimulation
Before stimulating the nerve directly, it’s important to consider what muscle(s) are innervated by the specific nerve and what functional assessment technique is being used (i.e. in-vitro, in-situ or in-vivo). For example, if you are interested in studying the mechanics of the tibialis anterior (TA; dorsiflexors) in-vivo, you could stimulate the sciatic nerve. However, the sciatic nerve has many branches to it that also innervate the antagonistic muscles (i.e. gastrocnemius, soleus, plantaris) and this could result in activation of BOTH the anterior and posterior compartment of the lower hindlimb and almost always end up as plantarflexion. Because of this, you would want to stimulate a branch of sciatic nerve closer to the muscle of interest. In this case it would be the common peroneal nerve which wraps around the knee joint then down the anterior part of the lower leg.
For nerve stimulation, the type of electrode is important to consider. There are several different types of electrodes that can be used, the most common are EMG style needle electrodes and nerve cuff/hook electrodes. In the scenario above, because the measurements will be done in-vivo, we would prefer to use the non-invasive needle electrodes placed on either side of the peroneal nerve.
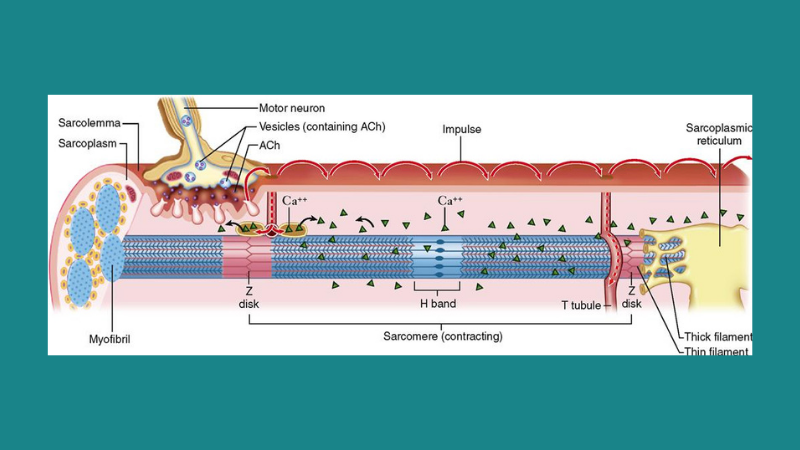
Once in position, stimulation parameters (frequency, duration, amperage) can be set, and an electrical stimulus is sent to the nerve. Stimulation depolarizes the motoneuron which travels along the axon to the neuromuscular junction (NMJ) and results in the release of acetylcholine (ACh) across the synaptic cleft. These neurotransmitters then bind the ACh receptors on the muscle’s sarcolemma which propagates along the sarcolemma to the T tubules and triggers release of calcium from the Sarcoplasmic Reticulum (SR). Calcium then binds troponin and activates the myofilament to induce contractions (Figure 1).
. Encyclopedia of Foods & Health.")
Figure 1: Motoneuron activation of muscle. Adapted from Khedkar et al. (2016). Encyclopedia of Foods & Health.
Stimulating the nerve is ideal for studying neuromuscular junction (NMJ) transmission, peripheral nerve regeneration or neurodegenerative disease whereby the functionality of muscle activation is the primary objective (i.e. motor neurons). Of particular interest is the ability to assess regeneration and innervation following treatment to see if newly formed NMJs are functional or measuring motor unit number estimate (MUNE). If a particular disease model doesn’t seem to have a nerve component, this type of stimulation can be used to get a sense of overall neuromuscular function.
Muscle Stimulation
In simplest terms, direct electrical stimulation of the muscle, via field or needle electrode, results in a very similar cascade of events as nerve stimulation. However, this process bypasses the motoneuron and depolarizes the sarcolemma directly to eliminate synaptic transmission as a factor in assessing muscle function. Using our earlier example of measuring TA (dorsiflexion) function in-vivo, needle electrodes are placed subcutaneously with the tips of the electrodes resting on the belly of the muscle or group of interest (Figure 2). Be mindful not to puncture the muscle tissue as this could result in damage to the fibers. In some cases, placing the electrodes at the proximal and distal end of the muscle will also work, but this will require higher amperage to fully stimulate the muscle and thus it is not recommended for dorsiflexion in-vivo, due to the likelihood of activating the antagonistic group. When measuring muscle function in-situ, electrode placement is quite similar to in-vivo. However, isolated muscle mechanics would make use of field stimulation using platinum-iridium electrodes in a tissue bath to generate a strong electric field which depolarizes the sarcolemma.
Direct muscle stimulation is incredibly useful when studying neuromuscular or neurodegenerative diseases where the quality or viability of the muscle is the primary detriment. In this instance, researchers may ask whether the muscle machinery still works or how it is affected in diseases such as Muscular Dystrophy, Aging or Cachexia. Or in other cases, injury to the muscle through volumetric muscle loss (VML) or ischemia/reperfusion (IR).
This is not to say that these disease or injury models lack a neurodegenerative component, in many cases they do (Sartori et al.)
But for many of these disease models, the researcher may be asking questions such as; does the muscle still contract and produce force or are there signs of atrophy? Are there disruptions in the myofilament that are hindering muscle function? etc.

Figure 2: Needle electrodes placed subcutaneously to directly stimulate dorsiflexor muscles. Courtesy Dr. Harun Noristani, Dr. Young-Jin Son Lab, Shriners Pediatrics Research Center.
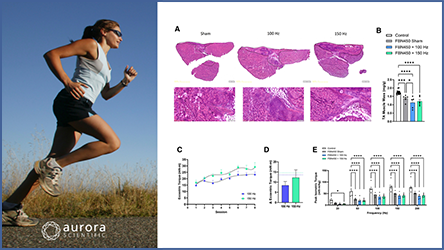
If you’re unsure of the effect of disease on the NMJ or motor neuron innervation, consider using both nerve and muscle stimulation to see if functional deficits differ between the two. Should your measurements indicate direct muscle stimulation produces greater force, there could be a neurodegenerative impact that is limiting transmission and activation of the muscle while the muscle architecture remains intact. This question is particularly important in neurodegenerative diseases such as ALS where the focus has been on the loss of motor neurons and less so on the functional deficits in muscle. Rizzuto et al. investigated this using an intact sciatic-soleus nerve-muscle preparation in-vitro and showed clear deficits in force production through both muscle and nerve stimulation in SOD1 mice (Figure 3A). Interestingly, force production via direct muscle stimulation was significantly higher than nerve stimulation in the diaphragm-phrenic nerve preparation and similar to WT (Figure 3B). This suggests the diaphragm muscle can maintain its functionality longer than hindlimb muscles, despite neuromuscular transmission detriments.
.")
Figure 3: Specific tetanic force measured from soleus and diaphragm intact nerve-muscle preparation. Rizzuto et al. JoVE (2017).
For more detailed information on making functional measurements as well as tips and tricks for using our 1300A system, be sure to check out our blog!
Featured Imaged from Basicmedical Key